FULLY SUGARED.
SUGAR.
FRUIT SUGAR.
CGM.
AN INTRODUCTION.

What role do carbohydrates play in our diet?
If we go back in time to when we still "lived in and from nature": When did carbohydrates exist and in what form? A few berry bushes in the forest? And when were they available as a food source? Maybe 2-3 months a year? And yes, that's right: that was before winter, a time when the supply of food was very low. So did it make sense to build up a small energy depot in the form of visceral fat ("floating tires") during this time? Most certainly. Does it make sense today to trigger this "fat building mechanism" 365 days a year? I'll leave the answer to you...
I am of the opinion that carbohydrates do not have a good energy balance. This statement sounds provocative in view of the fact that in moments of "weakness" we crave something sweet, something starchy: the chocolate (or muesli) bar between meals, the cake, the jelly babies, but also the pasta for lunch or the bread for dinner. These "sugar bombs" give us a short-term kick. Or not, because if you're honest with yourself, you'd prefer to lie down and sleep after a lunch of pasta, potatoes and the like, wouldn't you?
But watch out: Carbohydrates, sugar etc. have a lot of energy (calories!) ...?! Marathon runners need them, they fill their glycogen stores before the run! The brain only works with glucose, i.e. sugar! Or is it not that simple after all?

Sugar is bad, that's clear.
Fructose from fruit is the healthy alternative, isn't it?
Or: Why an apple is (biochemically speaking) twice as toxic as alcohol[1].
Fructose, which most nutritional guides refer to as "healthy sugar" and is almost always recommended, occupies a special position in carbohydrate metabolism. As the body cannot burn fructose directly, in simple terms it must first be converted into glucose. This takes place in the liver and the capacity for this process is quite low. Excess fructose is converted into fat deposits, which are stored in the liver. This leads to a fatty liver. Speaking of fatty liver: we know this from alcoholics. In this context, I would like to point out that the LD50[2] is a standardized toxicity index that indicates how much of a substance you have to ingest in order to die from it. This index exists for almost everything, including water, for example. For water, this value is 90g per kg of body weight. So I would have to consume around 7 liters of water to die from it. For refined household sugar the value is 30g / kg and for ethanol (alcohol) 7g / kg body weight. And here it comes:
The LD50 toxicity index of fructose is 4g / kg
i.e. in my case, around 30dag of pure fructose would be fatal.
In my opinion, these figures alone illustrate what a game with fire the consumption of fructose in the form of fruit, fresh fruit juices, corn syrup... is! Incidentally, regular consumption of fructose is also linked to fatty liver, cancer, metabolic syndrome, diabetes, cognitive decline, etc.[3][4]
[1] https://www.aatbio.com/resources/toxicity-lethality-median-dose-td50-ld50/fructose vs. www. aatbio.com/resources/toxicity-lethality-median-dose-td50-ld50/ethanol
[2] https://flexikon.doccheck.com/de/Therapeutische_Breite
[3] https://pubmed.ncbi.nlm.nih.gov/24257416/

Blood sugar measurements
Diabetes mellitus, affectionately known as "diabetes", is one of the most widespread diseases in the civilized world. The measurement of parameters that serve to diagnose this disease is therefore part of every "health check-up". There are different approaches.
Direct measurement in the blood
The measurement can be made either from capillary or venous blood and there are inexpensive devices for home testing. The amount of glucose currently present in the blood is measured. The guidelines recommend a value of <100 mg/dl on an empty stomach (i.e. after at least 8 hours without food) and <160 mg/dl 2 hours after a meal. In between, the value rises to over 200 mg/dl even in "healthy" people who "do everything right". I personally keep my fasting blood glucose below 85 mg/dl and normally don't want it to rise to more than 110 mg/dl after a meal.
Measuring HbA1c - the "long-term sugar"
The red blood cells (erythrocytes) and the haemoglobin they contain glycate at a fixed rate, i.e. in simple terms they bind to glucose. This effect is used in blood glucose measurement to compensate for the strong fluctuations in direct measurement. It is assumed that the erythrocytes have a fixed lifespan and the percentage of glycated hemoglobin is measured. This measurement therefore represents the average glucose value during the lifetime of the erythrocytes. The more sugar was present during this time, the more hemoglobin is glycated. A longer or shorter lifespan of the erythrocytes therefore also has an influence on the HbA1c. More on this elsewhere.
Measuring insulin
When glucose is in the blood, the pancreas releases the hormone insulin. This transmits the glucose to the cells where it is to be absorbed in order to be burned in the mitochondria as part of the respiratory chain to produce energy. The more glucose in the blood, the more insulin is on its way, provided the pancreas is functioning properly. The target value used by my laboratory is useless for my application, as can be seen in the graph: I try to keep my insulin value as low as possible. I will be happy to share the reasons for this below.
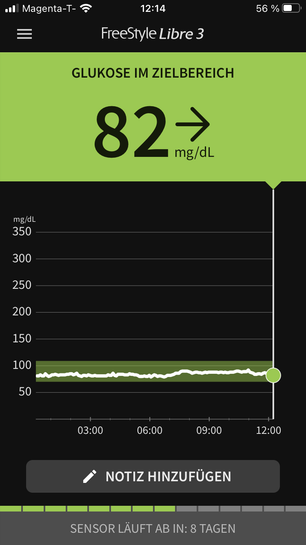
Continuous blood glucose monitoring with a CGM sensor
CGM is the abbreviation for CONTINUOUS GLUCOSE MONITORING. This refers to small "wearables", i.e. devices that can be worn on the body for a certain period of time. CGM sensors measure the glucose level at short intervals via the interstitial fluid. This correlates with the blood glucose level and, put simply, with a short time delay, the progression of the blood glucose can not only be recorded momentarily, but also automatically with the help of a smartphone. The sensors can usually remain on the body for around 14 days and then have to be replaced.
Disclaimer
The information and recipes contained on this platform and linked media reflect my personal experience only and are provided for informational purposes and as culinary inspiration. The recipes and nutritional information do not constitute medical advice, diagnosis or treatment and are not intended as a substitute for professional medical advice or treatment. Any recommendations reproduced in the media we maintain are not a substitute for advice from medical professionals or nutritionists. Readers with specific health concerns, food allergies, individual dietary needs or medical conditions should seek professional medical advice before implementing the recipes or dietary recommendations described herein. The author, publisher and operator of this platform accepts no responsibility for any health problems or damage that may arise from the use of the recipes or information contained on this platform. It is strongly recommended that you seek qualified medical advice or consult a nutrition specialist if you have any health concerns or before changing your current dietary habits. The authors and publishers of this media assume no liability for the accuracy or completeness of the information and recipes provided and it is the responsibility of the reader to take allergic reactions, food intolerances or other health concerns into account. Furthermore, neither the authors, publishers nor operators assume any guarantee or liability for the effectiveness of the measures presented. Zarastro GmbH is not responsible for the content of websites accessed via hyperlinks.